Slipped capital femoral epiphysis: Modern method of management
Introduction:
Slipped capital femoral epiphysis is one of the commonest adolescent hip disorders and a very common cause of early onset hip osteoarthritis. It is a traumatic or non-traumatic slippage of the femoral capital epiphysis over the metaphysis which leads to profound changes in the hip biomechanics, range of motion and vascularity.
Clinical features:
Typically seen in adolescent obese males
Endocrinopathies common
Chronic pain in the hip, thigh or knee followed by acute exacerbation with inability to bear weight (in some kids)
Out-toeing gait
External rotation deformity of the hip with restricted flexion
Diagnosis:
Plain X-rays:
Good quality plain radiographs of the pelvis with both hips- AP and frog leg lateral views are usually diagnostic of SCFE.
The classical signs of Klein’s line (line passing through the superior border of the neck passes through the superior part of the epiphysis), Trethowans sign, double density sign, etc. help in the diagnosis of SCFE.
Plain radiology is also helpful in classifying the slip (in most cases) and thus helps in planning the managements.
CT scans:
CT scans are very useful to exactly quantify the deformity in SCFE. Many a time, the exact grade of SCFE is underestimated on plain x-rays and CT scans help in deciding the plan for surgery.
MRI:
MRI can be used in some cases to know the vascularity of the femoral head pre-operatively so as to exactly prognosticate the patient.
Classification:
A) LODER’s stability classification:
Stable: Able to bear weight (AVN rate- 1%)
Unstable: Unable to bear weight (AVN rate- 60-80%)
Classification:
B) Temporal classification
Acute SCFE: Symptoms less than 3 weeks
Chronic SCFE: Symptoms more than 3 weeks
Acute on chronic SCFE: Chronic symptoms of more than 3 weeks followed by an acute exacerbation
C) Severity classification:
Mild: Displacement <30 degree
Moderate: Displacement 30-60 degree
Severe: Displacement> 60 degree.
Treatment:
The goals of treatment of SCFE are:
Prevention of further slippage by obliteration of the physis (growth plate)
Correction of the deformity, thus preventing FAI (impingement) and further degenerative joint disease
At the same time, maintenance of vascularity of the epiphysis (slipped head)
With these goals in mind, the treatment modalities for SCFE are as follows:
1) In-situ pinning: This involves screw fixation without correction of the slip by cannulated cancellous screws. This is reserved for mild and moderate slips though there are some proponents of
in-situ fixation for even severe slips.
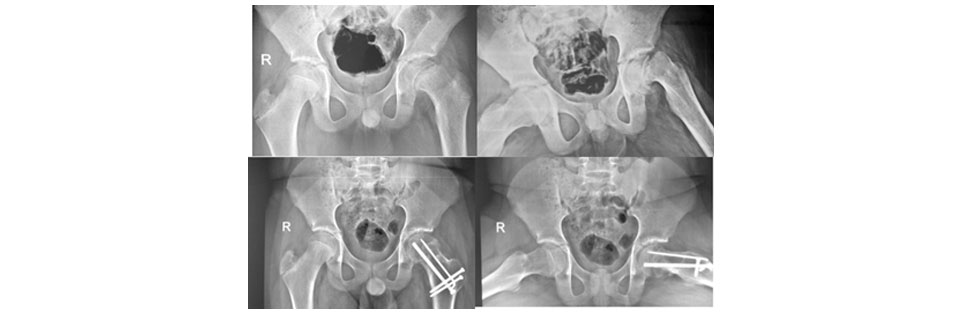
Figure 2: Showing Mild SCFE ® treated with in-situ cannulated cancellous screw fixation.
3)Femoral Neck osteotomy: This procedure involves correction of the deformity from the anterior approach. This, though is very robust in good correction of the deformity carries a very high risk of avascular necrosis.
4) In-situ pinning with proximal femoral osteotomy: This procedure involves in-situ pinning with correction of the deformity not at the site of the deformity but distally at the level of the intertrochanteric region.
5) Modified Dunn osteotomy (Dunn osteotomy through the safe surgical dislocation approach): The modified Dunn osteotomy described by Ganz and colleagues in 2009 has slowly become the treatment of choice for moderate to severe slips. It is an extremely technically demanding procedure, which can correct the deformity of SCFE right at the level of deformity without harming the vascularity of the capital femoral epiphysis. This procedure is followed at a few centers around the world which have the required training for the same and is associated with robust correction of the deformity with very low rates of AVN even in unstable slips.
Figure 2: Showing pre-operative and post-operative xrays of severe (L) unstable SCFE treated with modified Dunn osteotomy showing excellent healing and no signs of AVN at 2 years follow-up